Academic pharmacist Nataly Martini highlights the importance of understanding non-Hodgkin lymphoma and pharmacists’ roles in managing this condition
Friday 1 November 2024, 01:00 AM
14 minutes to Read
Website intended for a NZ health professional readership


Persistent pain affects physical, mental, social and spiritual wellbeing, and is one of the most prevalent long-term conditions in New Zealand. In this article, Vanessa Brown discusses persistent pain, including its causes, symptoms and treatments. She also explores the concept of central sensitisation and its role in persistent pain
Our suite of CLASS activities provides meaningful independent and peer group learning that you can put into action, while helping you complete your annual recertification requirements.
You can choose how many elements you wish to undertake, depending on your professional development plan, but it is recommended that you complete both CLASStime and CLASSact before CLASSmates.

This CLASStime article supports professional development with respect to:
As you read, highlight new knowledge or areas where you need to know more. You can also use the Capture button online to keep notes of your thoughts and reflections on this article. This may be useful if you choose to proceed to CLASSact and CLASSmates for this topic.
Completing this CLASStime activity may allow you to fulfil some or all of the following elements of your annual recertification requirements:
This activity has been endorsed by the Pharmaceutical Society of New Zealand as suitable for inclusion in a pharmacist's continuing education records for continuing professional development purposes.

As with so many other things in health, chronic pain has had a name change, and in 2020, the International Association for the Study of Pain (IASP) updated the definition to reflect changes in evidence and understanding. Chronic pain is now referred to as persistent pain, and we know this is a global crisis. We are all exposed to patients with persistent pain in our roles as pharmacists, so I do not need to tell you this condition is exceedingly difficult to manage and very time consuming.
Just under 800,000 New Zealanders were living with persistent pain in 2016, and this is expected to increase to 1.3 million by 2048 as the population ages. The current cost of persistent pain to society is higher than that of diabetes and heart disease, and this is predicted to rise to $24 billion by 2048.1 This includes burden of disease costs, indirect costs, and direct costs to Te Whatu Ora – GP appointments, emergency department visits, hospital admissions and bed days, as well as imaging studies, medications and diagnostics relating to pain.
Add to this the issues that pain is disproportionately more prevalent in Māori, Pacific and women, and is also an independent driver of poverty, and we start to understand the magnitude of the issue.
New Zealand data have shown that Pacific and Asian patients are less likely to attend “chronic pain” services than Europeans, while Māori, Pacific peoples and, to a lesser extent, people of Asian descent present to these services with a higher impact of pain.2
In addition, there are inequities in the efficacy of treatment, with Māori, Asian and Pacific peoples experiencing poorer outcomes at discharge and/or follow-up than Europeans. These findings are more prominent for outcomes relating to mental health and pain beliefs, rather than pain and physical function.3
These studies highlight that “different cultures have different beliefs and frameworks for experiencing, interpreting and managing pain, some of which may clash with the biopsychosocial framework currently implemented by pain management clinics”.3
For example, whānau/family and spirituality are integral components of health for Māori, Pacific peoples and a number of Asian cultures. Cultural influences may also make Māori, Pacific and Asian peoples less likely to reveal their pain to others. All this affects the decision to seek treatment and who to seek treatment from.2,3
In addition, barriers to healthcare are well known for Māori and Pacific peoples in New Zealand, including language and communication, financial cost and transport. There is also the possibility that unconscious bias, stereotyping or a lack of understanding of different cultural views surrounding pain may limit referral for further treatment.2,3
We all know persistent pain is hard to treat. These are complex people with complex needs. Over 75 per cent of patients also have mental health issues or complex medical comorbidities, and a traditional biomedical approach does not work – an innovative and interdisciplinary approach is required.
Pain is a universal experience that is essential for survival. It is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage. As mentioned, the IASP updated its definition of pain in 2020. The new definition (see panel below) emphasises that pain is a subjective experience influenced by biological, psychological and social factors.4
Persistent pain is defined as pain that lasts beyond the expected time for tissue healing, or pain that is associated with a chronic medical condition. It can be characterised by a range of sensations, including throbbing, aching, burning, shooting or stabbing. Persistent pain can also have a significant impact on a person’s quality of life, affecting their physical, emotional and social wellbeing.
Persistent pain is a complex condition that involves multiple factors, including biological, psychological and social factors. It can be caused by changes in the nervous system that lead to a state of hyperexcitability, known as central sensitisation. Central sensitisation is a process in which the central nervous system becomes more sensitive to pain signals, leading to an amplification of pain perception. It is an important concept in the understanding of persistent pain and is covered in more detail later in this article.
“An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.”
Six additional notes:
Persistent pain can be caused by a variety of factors, including injury, illness and disease. Common causes of persistent pain include:
The symptoms of persistent pain can vary depending on the cause and location of the pain. Common symptoms include pain that:
As an undergraduate, my total understanding of pain revolved around the WHO three-step analgesic ladder for adult cancer pain, which is a fabulous tool for what it is (see Figure A1.1 in Annex 1 of the WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents; tinyurl.com/WHO3step).5 However, this ladder is not appropriate for treating adult non-cancer pain.
In 2010, neurobiologist Clifford Woolf published new evidence which changed the way we think about pain and, hence, how we treat it. We now know that there are four main categories of pain (Figure 1).6
Nociceptive pain – the “common” pain experience, where a noxious stimulus (heat, cold, intense force, etc) stimulates the nociceptor sensory neuron. We are immediately aware of the pain and withdraw from the stimulus. This is a protective response to high-threshold pain.
Inflammatory pain – as the name suggests, this is caused by activation of the inflammatory response due to tissue damage or infection. This is more likely to be low-threshold pain, and the tenderness promotes repair within the tissues.
Pathological pain is not protective and is separated into two classes:
Neuropathic pain – this is a result of nerve damage and causes abnormal central processing within the nervous system, which causes altered sensations.
Nociplastic pain – initially classified as dysfunctional pain, nociplastic pain is the most common type of pain that patients present with at the “chronic pain” clinic.
The IASP has defined nociplastic pain as: “Pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors, or evidence for disease, or lesion of the somatosensory system causing the pain.”4
So, despite our best efforts to find a cause through blood work and imaging, all appears “normal” from a biomedical perspective, yet the patient has significant and persistent pain.
Figure 1. Pain can be broadly divided into four categories: (A) nociceptive pain represents the sensation associated with the detection of potentially tissue-damaging noxious stimuli and is protective; (B) inflammatory pain is associated with tissue damage and the infiltration of immune cells and can promote repair by causing pain hypersensitivity until healing occurs; (C) pathological pain is a disease state caused by damage to the nervous system (neuropathic pain) or by its abnormal function (dysfunctional or nociplastic pain)
Treating persistent pain is a complex situation, where we must balance pain, quality of life, comorbidities, medication doses, interactions and medication side effects.
Medications should be considered third-line treatment for persistent pain, following physical activity and counselling/psychology support. The gold standard for treating persistent pain is a 50 per cent reduction in pain score; however, many guidelines are written with evidence for treatments that have only managed to achieve a 30 per cent reduction. The focus is more on quality of life, and pain score is only one area that is assessed.
As persistent pain requires a holistic approach, we use the electronic Persistent Pain Outcomes Collaboration (ePPOC) assessment process in New Zealand – ePPOC is an independent platform developed and maintained by the University of Wollongong in Sydney (uow.edu.au/ahsri/eppoc). All 72 pain management providers in Australasia use ePPOC as their data capture platform, which enables outcomes to be benchmarked against other services.
This assessment involves:
Figure 2 shows ePPOC results for a patient before and after involvement in a pain clinic.
Figure 2. ePPOC results for a patient before and after involvement in a pain clinic
It is important to appreciate the limited role medications play and, if possible, select an agent that may cover multiple symptoms to reduce medication burden and lower the risk of adverse effects.
As you can see from the pain descriptions above, nociceptive pain is normally acute and can be managed with short-term options such as paracetamol or opioids. NSAIDs are indicated for acute injury or longer-term inflammatory conditions, such as arthritis. However, often these agents are contraindicated due to renal function, cardiovascular risk or concurrent long-term medications, such as anticoagulants.
For long-term conditions where inflammation is confirmed (inflammatory pain), steroid injections can be useful – directly into the joint or area affected. These injections can also be used to help with the differential diagnosis of an underlying inflammatory response or nociplastic pain.
Neuropathic pain is treated with agents that target the central nervous system, so commonly antidepressants or antiseizure medications (Table 1). The most commonly used agents in New Zealand are amitriptyline, nortriptyline, gabapentin, pregabalin and venlafaxine, with some second-line evidence for capsaicin cream, and third-line evidence for medicinal cannabis products (covered later).
Paracetamol, NSAIDs, capsaicin, opioids and cannabinoids work by inhibiting ascending pain transmission from the nociceptor sensory neuron to the somatosensory cortex, while antidepressants, antiseizure medications and cannabinoids facilitate descending pain modulation.
Table 1. Recommended pharmacotherapy for treatment of neuropathic pain
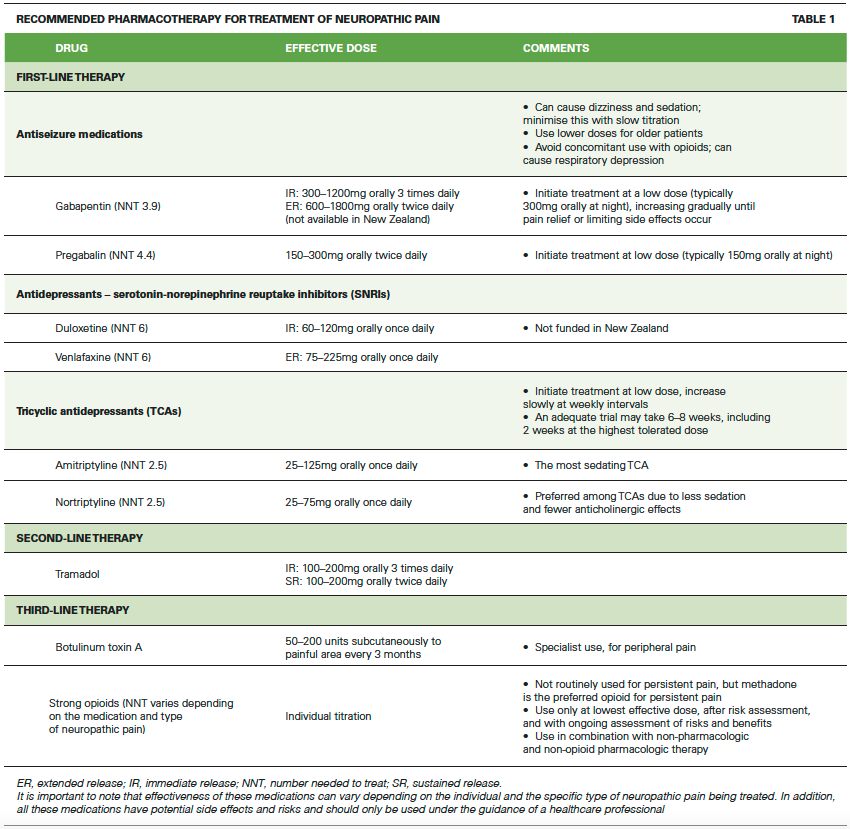
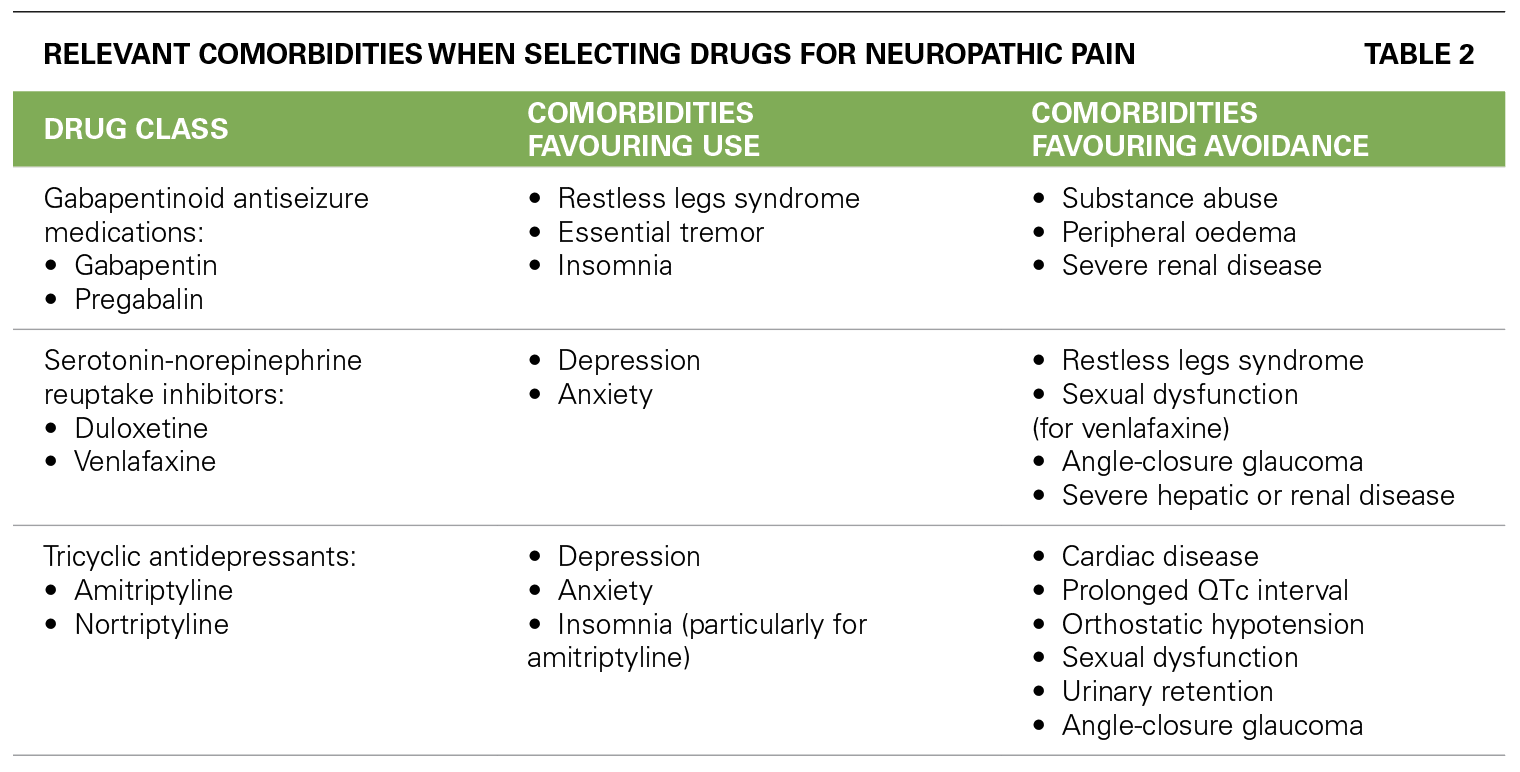
Table 2 shows some of the comorbidities that may be considered when selecting drugs for the treatment of neuropathic pain. In addition to comorbidities, the choice among treatments should be individualised based on the pain aetiology (if known), the patient’s age, concurrent medications, medication side-effect profile, cost, and patient preference regarding dosing frequency.
Table 2. Relevant comorbidities when selecting drugs for neuropathic pain
Nociplastic pain is by far the most complex to treat as there are no known stimuli, an inflammatory component has been ruled out, and there is no evidence of nerve damage. Despite that, the patient has persistent pain which affects their quality of life.
One area of evidence which helps explain this process is the concept of central sensitisation (see below). The Central Sensitisation Inventory (CSI; tinyurl.com/CSIworksheet) is a useful diagnostic tool to identify whether the patient is experiencing central sensitisation and to what extent.7 This is quite often a “lightbulb” moment in the consultation, when the patient feels validated. For many, this is the first time they realise it is not “all in their head”.
Opioids often make central sensitisation worse and can increase the level of central sensitisation more rapidly. The sooner appropriate treatment with antidepressants/antiseizure medications is started, the faster central sensitisation improves.
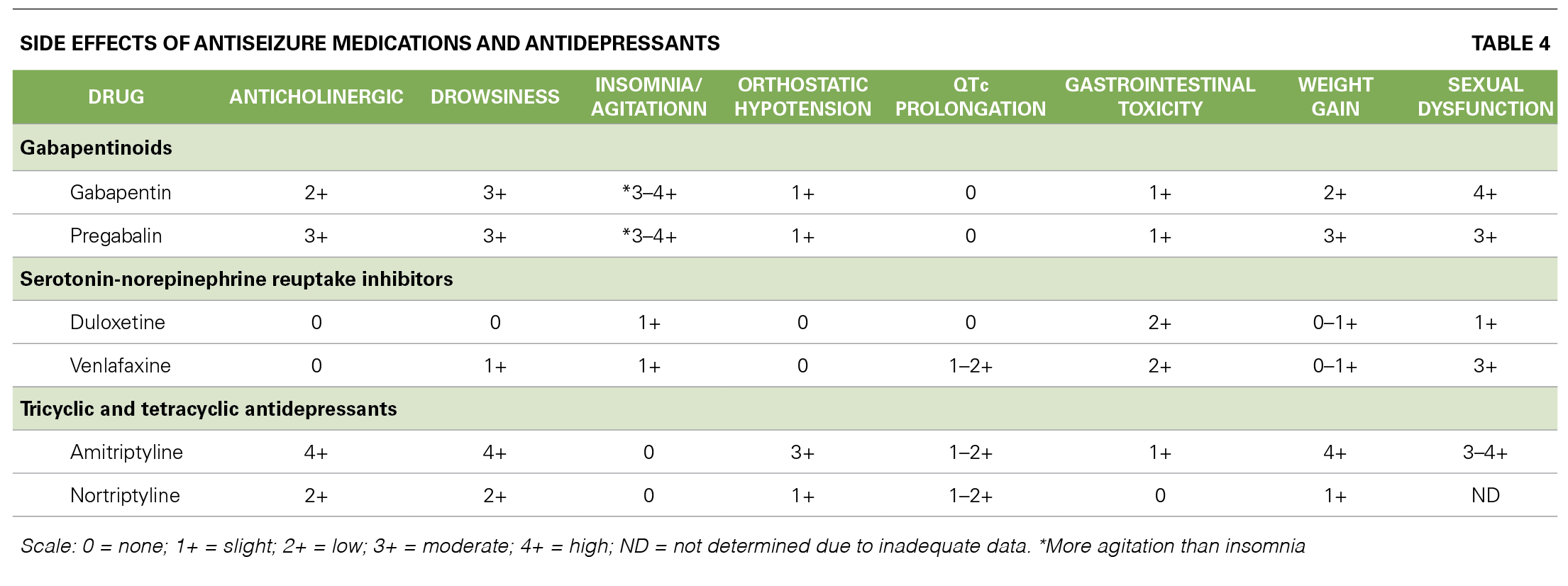
Table 3 helps summarise which pharmacological treatment we should consider for each type of pain. The goal is always to use the lowest possible dose for the shortest period of time. However, in persistent pain, the need for medications is often long-term and, in some cases, lifelong. So, it is important to know the different side-effect profiles of the medications (Table 4). As for all treatment options, we must balance the risks and benefits. Agents that commonly cause daytime sedation, weight gain, sexual dysfunction and anticholinergic effects can contribute significantly to a poor quality of life.
Note that patients can have a mixture of different types of pain (eg, nociceptive and nociplastic pain), which is when different pharmacological agents are indicated in combination (eg, NSAID and antidepressant/gabapentinoid).
Table 3. Summary of pharmacological treatment based on type of pain
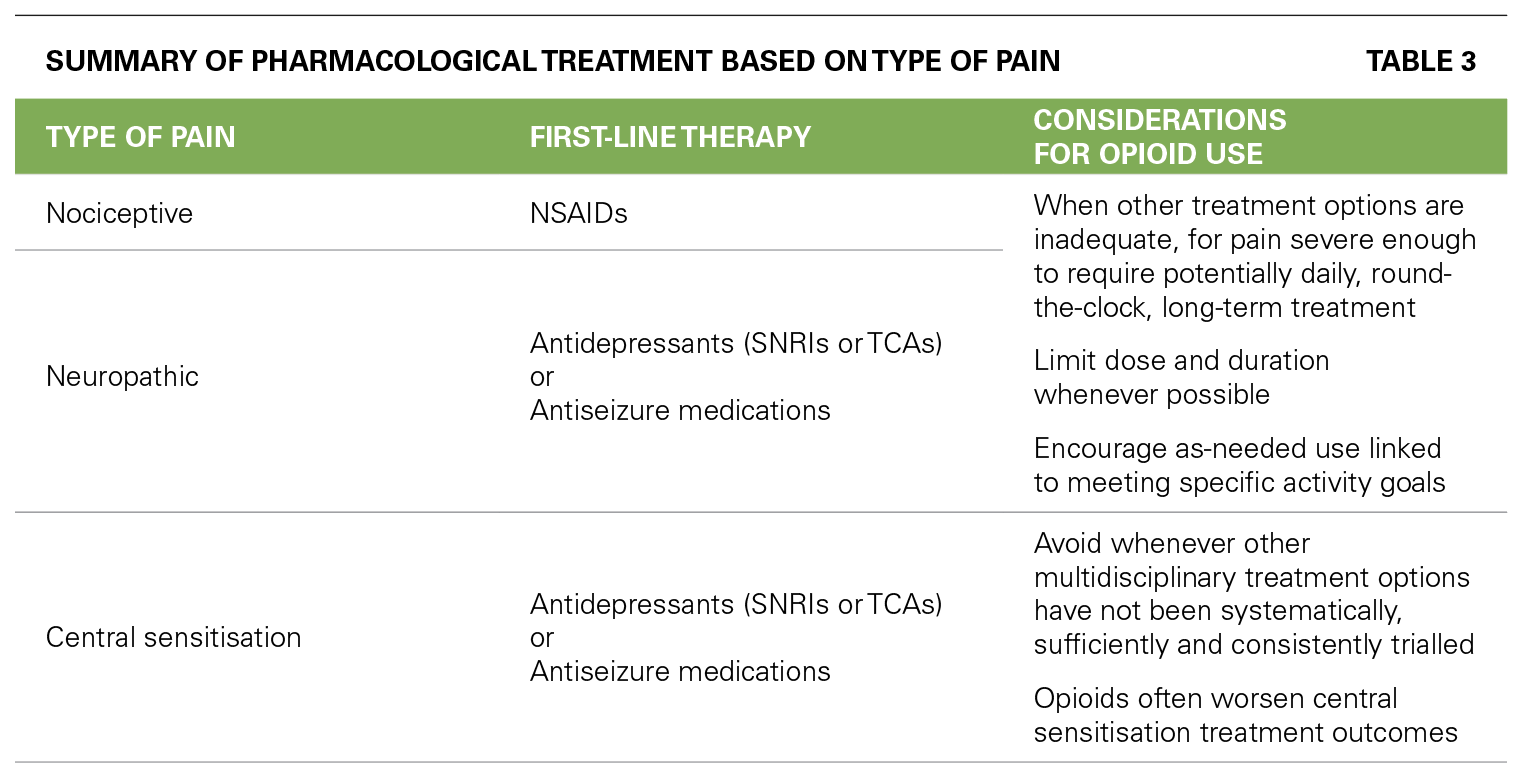
Table 4. Side effects of antiseizure medications and antidepressants
Central sensitisation is a process in which the central nervous system becomes more sensitive to pain signals, leading to an amplification of pain perception. This process can play a significant role in the development and maintenance of persistent pain.
Central sensitisation can be due to a combination of long-term pain and other stresses or can start from an injury or illness. It normally develops after having pain for more than 12 months.
In central sensitisation, the threshold for activation of pain fibres is lowered, and the amplification of pain signals occurs in the central nervous system. This results in an increase in pain sensitivity and a decrease in pain tolerance. The mechanisms underlying central sensitisation are complex and involve changes in the structure and function of the nervous system.
One of the primary mechanisms involved in central sensitisation is the release of excitatory neurotransmitters, such as glutamate and substance P, in the spinal cord and brain. These neurotransmitters activate pain pathways and cause the amplification of pain signals. Additionally, the release of inflammatory mediators, such as cytokines, can contribute to central sensitisation.
Central sensitisation can also result in changes in the way the brain processes sensory information, leading to altered perceptions of pain.
For example, in individuals with persistent pain, the brain’s pain processing centres may become more active, resulting in a heightened perception of pain. Additionally, central sensitisation can lead to the development of allodynia and hyperalgesia:
Central sensitisation can also contribute to the development of comorbid conditions, such as depression and anxiety. The emotional distress caused by persistent pain can activate the stress response, leading to the release of stress hormones, such as cortisol. These hormones can further sensitise the nervous system and contribute to the development of central sensitisation.
Treatment for central sensitisation typically involves addressing the underlying cause of the persistent pain and targeting the mechanisms involved in central sensitisation. This may include medications that target the release of excitatory neurotransmitters, such as N-methyl-D-aspartate (NMDA) receptor antagonists. Additionally, non-pharmacological interventions, such as cognitive behavioural therapy, may be helpful in reducing the emotional distress associated with persistent pain and decreasing the impact of central sensitisation.
Completing the CSI during the initial triage and again 12 months later can be extremely useful to monitor the outcomes for that individual.
The 2018 “Simplified guideline for prescribing medical cannabinoids in primary care” addressed cannabinoid use in neuropathic pain, recommending against medicinal cannabinoids as first-line or second-line therapy, owing to limited benefits and high risk of harms.8 Although our evidence base for this is still from recreational products and synthetic cannabinoids, the risk of harm in medicinal products is actually very low.
The guideline suggests clinicians could consider medicinal cannabinoids for refractory neuropathic pain with multiple considerations, including a reasonable therapeutic trial of three or more prescribed analgesics first.
It was noted that when including all types of neuropathic pain, cannabinoids provide meaningful (≥30 per cent pain reduction) relief in chronic neuropathic pain for about 39 to 40 per cent of participants.
In practice, I have used medicinal cannabis products as a third-line or fourth-line option in hundreds of patients since it was legalised in New Zealand in 2017. I have seen benefit from using full-spectrum cannabidiol (CBD) oil and full-spectrum tetrahydrocannabinol (THC) oil in combination. Cost is the biggest barrier to this treatment option, with the “average dose” combination costing approximately $260–300 per month.
I prefer to use the two products separately to individualise the dose for each patient. Full-spectrum CBD oil appears to help with sleep, mood, anxiety, gastrointestinal issues, muscle spasms and quality of life. Generally, this needs to be combined with a small dose of full-spectrum THC oil to improve pain and central sensitisation.
Initially, the most important role as a pharmacist is to understand the different types of pain and what medications are indicated, what the therapeutic dose range is and how long it is expected to take to notice a therapeutic benefit.
When a patient with acute pain is still struggling with symptoms six months later, discuss the concept of a pain clinic referral, as dealing with these symptoms at six to 12 months is much easier than five to 10 years after pain started.
Pharmacists play a key role in supporting both patients and prescribers in up-titrating medications, counselling about time to effect and adverse effects, as well as managing combinations of medications. It is also important to understand the need to review medications regularly and to wean/discontinue medications that have not shown a benefit after a reasonable time at a therapeutic dose.
The pharmacist role as part of the pain team mostly consists of deprescribing medications, explaining how different medications work for different types of pain, and building a rapport with the patient so they feel comfortable to ask questions. This is particularly important for people from ethnic groups where communication barriers may exist.
Cultural safety is important and incorporating traditional medical practices into pain management should be considered when they are concordant with evidence-based guidelines. A key component of persistent pain management is patient education – this could highlight aspects of management that align with cultural practices or beliefs, as well as identify those that are contradictory. The support of whānau/family or other health advocates can also be proactively recommended.2,3
As we continue to struggle with inequity and access issues, many patients will present at a pharmacy for help before they present at a doctor, and some will self-medicate with general-sale analgesia for months or years before ever seeing a health professional. This poses a huge risk and contributes to our growing inequity issues and emergency department presentation rates. Knowing the funding streams and how these patients can receive better and more affordable access to services is key.
Vanessa Brown is a clinical pharmacist who has completed postgraduate studies in palliative care, clinical pharmacy and pain management. She currently works in Hawkes Bay as part of a multidisciplinary chronic pain team

Please CAPTURE this article before leaving this page. To move on to CLASSact, where you can download an interactive PDF that provides you with both knowledge and reflective questions for independent learning, click the button below.
Completing this CLASSact worksheet may allow you to fulfil some or all of the following elements of your Pharmacy Council annual recertification requirements:

Please CAPTURE this article before leaving this page. To move on to CLASSmates, where you can download a peer group meeting guide and activity tool based on CLASStime and CLASSact, click the button below. It includes a facilitator guide, user guide, notes template and Jamboard tool (for online meetings).
Completing this CLASSmates activity may allow you to fulfil some or all of the following elements of your Pharmacy Council annual recertification requirements:

1. Moore D, Davies P. The Problem of Chronic Pain and Scope for Improvements in Patient Outcomes. Sapere Research Group, October 2018.
2. Lewis GN, Upsdell A. Ethnic disparities in attendance at New Zealand's chronic pain services. N Z Med J 2018;131(1472):21–28.
3. Lewis G, Borotkanics R, Upsdell A. Inequity in outcomes from New Zealand chronic pain services. N Z Med J 2021;134(1533):11–20.
4. International Association for the Study of Pain. Terminology.
5. WHO. Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents. 2018.
6. Woolf CJ. What is this thing called pain? J Clin Invest 2010;120(11):3742–44.
7. Neblett, R. The central sensitization inventory: A user’s manual. J Appl Behav Res 2018;23:e12123.
8. Allan GM, Ramji J, Perry D, et al. Simplified guideline for prescribing medical cannabinoids in primary care. Can Fam Physician 2018;64(2):111–20.
Academic pharmacist Nataly Martini highlights the importance of understanding non-Hodgkin lymphoma and pharmacists’ roles in managing this condition
Talking about butt stuff in the pharmacy can be awkward. Care Pharmaceuticals and Rectogesic® can help you get to the bottom of the issue